Nursing care plans are the backbone of the professional nursing practice. They help translate the clinical judgment into structured patient-centered action and ensure continuity, safety, and accountability across the healthcare settings.
Despite their importance, care plans are often misunderstood or treated as a documentation task rather than a critical tool.
According to studies published in The Journal of Nursing Administration, structured nursing care planning is associated with up to 25-30% improvement in patient outcome consistency, especially in the acute and chronic care settings.
Furthermore, the hospitals that focus on creating standardized nursing care plans report lower adverse event rates and improved communication.
This ultimate guide provides a comprehensive overview of the evidence-based Nursing Care Plans. We will delve into what they are, why they matter, and how to write effective NCPs.
So come on! Let’s get into it.
What is a Nursing Care Plan?
| A nursing care plan is a systematic, individualized plan of care that helps understand a patient’s unique health needs. |
According to the American Nurses Association (ANA), a nursing care plan is a dynamic document that guides nursing care. Furthermore, it supports critical reasoning and promotes patient safety.
Furthermore, care plans operationalize the nursing process to make sure that the assessment findings lead to meaningful evidence-based nursing actions.
Also, it contributes to the:
- Nursing diagnoses
- Desired Patient Outcomes
- Planned Nursing Interventions
- Rationales for interventions
- Evaluation of outcomes.
Different Types of Nursing Care Plans
Care plans can be both informal and formal. And there is a little difference between them. While informal plans are mostly the strategies that exist in the nurse’s mind, the formal ones are written based on the patient’s care information.
Furthermore, formal plans are further classified into two different categories; they include:
- Standardized Care Plans: They specify nursing care for groups of clients and address their everyday needs. Moreover, they are for those with a specific condition.
- Individualized Care Plans: These plans are mostly tailored according to the patient’s needs, health conditions, and other details, which are not highlighted in standardized care plans.
Following the nursing care plans is essential to provide better healthcare to cater to the unique patients’ needs and reduce errors.
Why Do Nursing Care Plans Matter in Professional Settings?
Nursing care plans are essential to ensure that patient-centered care is provided. Furthermore, it helps maintain continuity, improve the outcomes, and reduce the errors.
Come on! Let’s dive deep into the details.
Improved Patient Outcomes
Evidence shows that structured care planning improves outcomes. A multi-center study of medical surgical units found that patients whose care was based on the formal NCPs showed:
- 22% medication errors
- 18% reduction in the hospital-based complications
- Shorter average of stay to 0.5 – 1.5 days.
Continuation & Coordination of Care
Nursing care plans serve as a communication bridge between nurses, physicians, and other healthcare professionals. Well, this is very essential in shift changes, transfers, and interdisciplinary rounds.
Legal and Professional Accountability
If we look from the regulatory point of view, the nursing care plans serve as the legal documentation that shows the critical judgment, adherence to standards, and patient advocacy.
Additionally, failure to maintain accurate care plans has been cited in malpractice cases as evidence of substandard nursing practice.
Support for Evidence-Based Practice
Modern care plans incorporate current clinical guidelines, standardized nursing language, measurable outcomes, and more, which reinforces evidence-based nursing.
In short, the nursing care plans are the proactive tools that can directly impact the patient outcomes.
The Nursing Process – The Foundation of the Care Planning
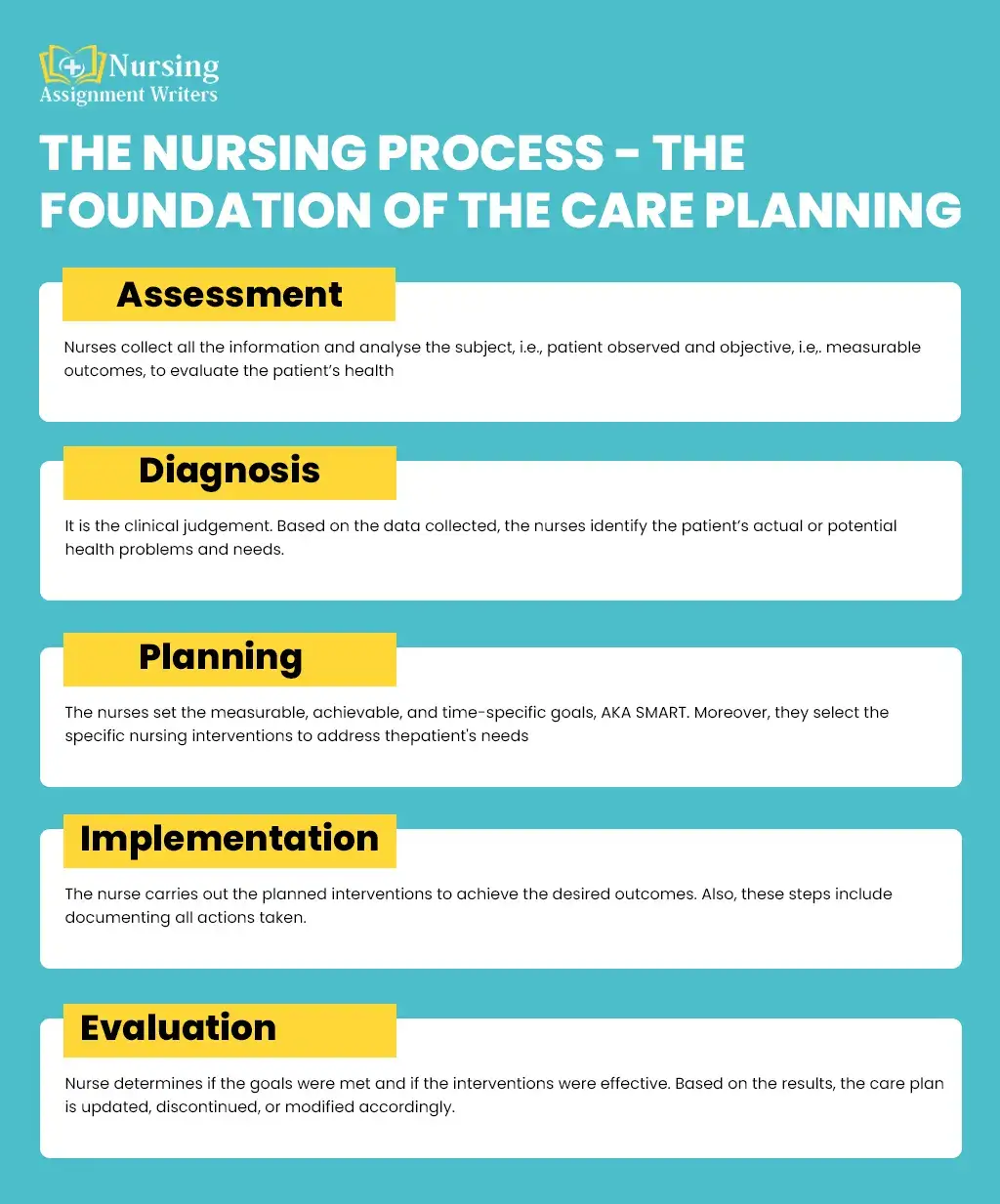
The nursing care plan follows the five steps of the nursing process:
- Assessment
- Diagnosis
- Planning
- Implementation
Come on! Let’s dive deep into them:
- Assessment: Think of it as a data collection step. Here, the nurses collect all the information and analyze the subject, i.e., patient observed and objective, i.e,. measurable outcomes, to evaluate the patient’s health. This helps them in creating the best healthcare plans.
- Diagnosis: It is the clinical judgement. Based on the data collected, the nurses identify the patient’s actual or potential health problems and needs. Furthermore, this includes analyzing the data to create nursing diagnoses, for example, the risks and benefits.
- Planning: The third step is to plan. The nurses set the measurable, achievable, and time-specific goals AKA SMART. Moreover, they select the specific nursing interventions to address the patient’s needs.
- Implementation: The nurse carries out the planned interventions to achieve the desired outcomes. Also, these steps include documenting all actions taken.
- Evaluation: Lastly, the nurse determines if the goals were met and if the interventions were effective. Based on the results, the care plan is updated, discontinued, or modified accordingly.
Using this standards-based approach ensures consistent evidence-based care and provides room for improvements as the patient’s condition changes.
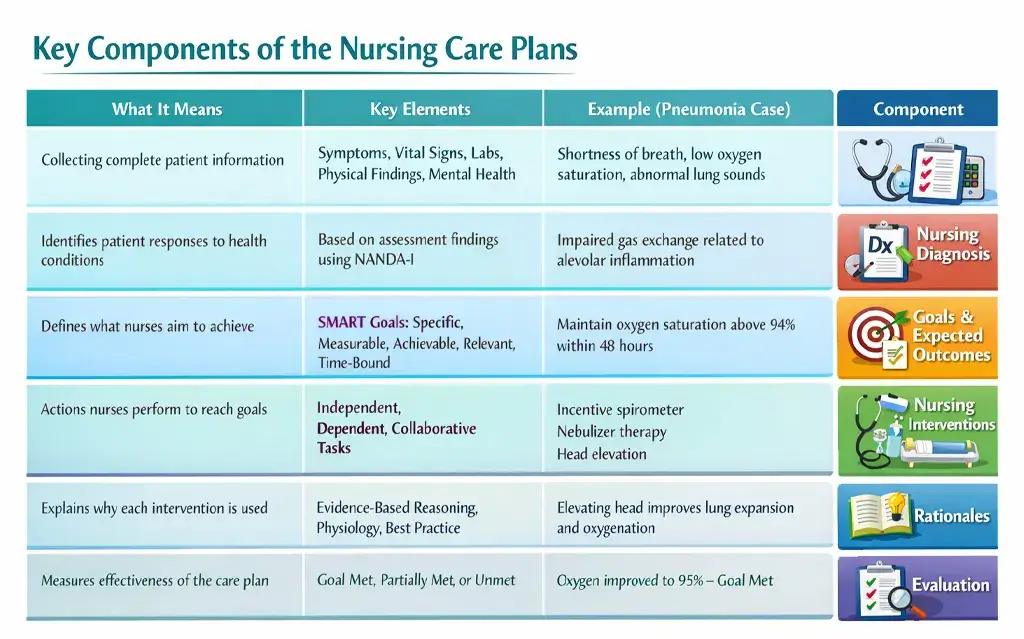
Key Components of the Nursing Care Plans
The nursing care plan includes six main components based on professional standards and frameworks. They include:
- Assessment Data
- Nursing Diagnosis
- Goals and Expected Outcomes
- Nursing Interventions
- Rationales
- Evaluation
Come on! Let’s dive deep into each of these components and discover how they can assist you:
1. Assessment Data
Patient health assessment and diagnosis are the first steps in developing a care plan. From subjective to objective and psychological data, nurses need to collect everything. For example:
- Patient’s symptoms?
- Vital Signs
- Lab
- Physical Findings
- Mental Health
This helps them create better nursing care plans. However, when assessing, nurses have to be careful as an inaccurate assessment can often lead to ineffective plans or medical errors.
Nursing Diagnosis
Nursing diagnoses differ more from medical diagnoses. Instead, they focus on human responses to health conditions. Furthermore, it is more of a statement that describes the patient’s health or concerns.
This is mostly based on the information gathered during the assessment. Many professional care plans use the NANDA-International (NANDA-I) nursing diagnoses.
Let’s dive deep into the depths by looking at the example of a real-world scenario:
Example
| Medical Diagnosis | There is the case of Pneumonia |
| Nursing Diagnosis | The Assessment includes the impaired gas exchange related to the alveolar inflammation as evidenced by dyspnea and low oxygen saturation. |
Proper diagnosis ensures that patients get healthcare help as needed.
Goals and Expected Outcomes
Think of them as the expected outcomes that will be achieved through the nursing interventions. While these goals can be long-term or short-term, the nurses need to follow the SMART framework. They must be:
- Specific
- Measurable
- Achievable
- Relevant
- Time Bound
Following the example of pneumonia, here are the goals.
Example of Expected Goals
The patient will maintain oxygen saturation above 94% on room air within the next48 hours.
Additionally, the research shows that the care plans with clearly measurable outcomes are more likely to show 40% of the documented improvements.
Nursing Interventions
Once the goal is set, the nurses will take the specific actions to address the nursing diagnosis. This will help them achieve the expected outcomes.
Additionally, they may be:
- Independent tasks that are initiated by the nurses
- Depended, also known as provider-ordered
- It is mostly the interdisciplinary decision of both patients and nurses.
For Examples:
To enhance the outcomes of the pneumonia case, here is what nurses can do:
- Encourage deep breathing exercises, coughing, and use of an incentive spirometer every hour while awake/
- Use nebulizer treatments to help loosen thick secretions
- Performing suction if the patient is unable to clear secretions independently.
- Elevate the head of the best to a semi-fowler’s or high-Fowler’s position to maximize lung expansion.
These interventions can help nurses provide better healthcare to the patient and achieve measurable outcomes without any problems. However, these treatment plans may vary depending on the causes and the problems.
Rationales
Rationales explain why each of the interventions is performed. Furthermore, it links the practice to psychology or evidence-based guidelines. Also, each of them has the proper explanation, so the readers can understand what you are talking about.
The perk of this rationale includes:
- Enhanced critical thinking
- Moreover, it supports the clinical education
- Also, it improves the quality of the documentation.
Evaluation
Lastly comes the evaluation. Think of it as a final conclusion that determines whether the goals were completely met, partially met, or unmet. Furthermore, if the outcomes are not achieved,d the nurses must:
- Reassess the patient
- Furthermore, they should modify the diagnoses or goals
- Even adjusting the interventions can help them enhance the outcomes.
By following through with all of this, nurses can provide better healthcare to the patients, and it even reduces the chances of medical errors. This reinforces that nursing care plans are living documents and not some static paperwork.
Sample Nursing Care Plan
To help you understand the Nursing Care Plan better, we have created a sample using a real-world scenario.
Let’s dive into it.
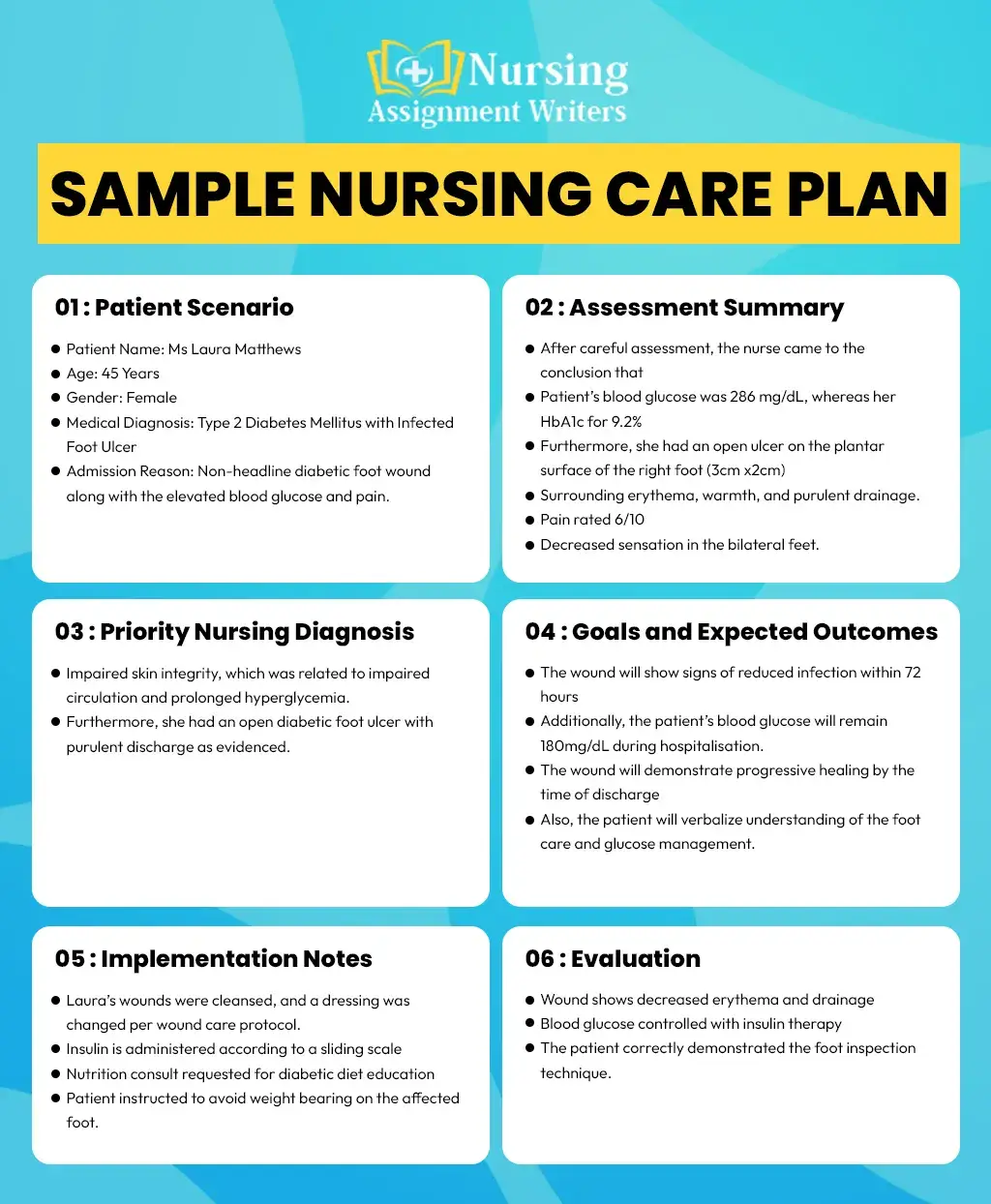
Patient Scenario
XYZ hospital receives the case of Ms Laura Matthews. She is 45 years old and a patient of Type 2 Diabetes. Recently, she was diagnosed with an infected foot ulcer. Here are the complete details:
- Patient Name: Ms Laura Matthews
- Age: 45 Years
- Gender: Female
- Medical Diagnosis: Type 2 Diabetes Mellitus with Infected Foot Ulcer
- Setting: Medical Surgical Unit/Wound Care
- Admission Reason: Non-headline diabetic foot wound along with the elevated blood glucose and pain.
Assessment Summary
The nurse assigned to Laura conducted both subjective and objective assessments to learn more about the patient’s health.
This includes:
Subjective Data:
According to the patient:
- My foot has been hurting more for the last few days.
- I don’t always check my sugar as I should do
- She even reports numbness and tingling in both feet.
Objective Data:
After careful assessment, the nurse came to the conclusion that
- Patient’s blood glucose was 286 mg/d,L whereas her HbA1c for 9.2%
- Furthermore, re she had an open ulcer on the plantar surface of the right foot (3cm x2cm)
- Surrounding erythema, warmth, and purulent drainage.
- Pain rated 6/10
- Decreased sensation in the bilateral feet.
The purpose of using both the subjective and objective care plans was to provide Laura with the best care plan.
Priority Nursing Diagnosis
After the careful assessment, the nurses were able to diagnose that Laura had:
- Impaired skin integrity, which was related to impaired circulation and prolonged hyperglycemia.
- Furthermore, she had an open diabetic foot ulcer with purulentdischargee as evidenced.
Goals and Expected Outcomes
After assessment and diagnosis, the next step was for the nurse to create the goals using the SMART framework. She created both the long-term and the short-term goals, such as:
Short-Term Goals:
- The wound will show signs of reduced infection within 72 hours
- Additionally, the patient’s blood glucose will remain 180mg/dL during hospitalisation.
These short-term goals made sure that the patient would be looked after during her time in the hospital.
Long-Term Goals
The long-term goals included:
- The wound will demonstrate progressive healing by the time of discharge
- Also, the patient will verbalize understanding of the foot care and glucose management.
Implementation Notes
Here is how the nurses implemented their care plan:
- Laura’s wounds were cleansed and a dressing was changed per wound care protocol.
- Insulin is administered according to a sliding scale
- Nutrition consult requested for diabetic diet education
- Patient instructed to avoid weight bearing on the affected foot.
Evaluation
After the careful analysis, the nurse evaluated:
- Wound shows decreased erythema and drainage
- Blood glucose controlled with insulin therapy
- The patient correctly demonstrated the foot inspection technique.
Here is what the care plan status showed:
Continuity of the wound care and glucose monitoring is essential. Furthermore, the nurses should reinforce the education to the patient prior to discharge so that they can take care of their wound at home. This will ensure that they have recovered property.
Struggling With Nursing Care Plans? Get Expert Help Today!
If you are facing troubles with your nursing care plans, we’ve got you. With us, you can save time, reduce stress, and submit well-structured nursing assignments with help from professional nursing writers.

Why Does This Care Plan Reflect Real Practice?
In short, this plan is perfect to:
- Address the chronic disease management
- Integrate wound care and metabolic control
- Emphasize patient education and prevention
- Use the practical bedside intervention.
The care plan may differ based on the patient’s age, medical condition, and outcomes. However, this is the standard process that every nurse has to follow while creating the perfect nursing care plans and receiving the desired outcomes.
Challenges in Nursing Care Planning
Even though the nursing care plan has proven its value in improving patient outcomes, they continue to face significant challenges in real-world clinical settings, for example:
- Time Constraints: One of the most frequent challenges in nursing care planning is the time constraints. High patient acuity, patient-to-nurse ratios, frequent admissions and discharges, and an extensive process of documentation significantly reduce the time nurses can devote to developing and updating comprehensive care plans. Additionally, in fast-paced environments such as emergency departments, intensive care units, and medical-surgical floors, nurses are often required to prioritize immediate clinical interventions over documentation. Thursdays care plans may be updated minimally, which limits their usefulness as real-time guides.
- Perception as Paperwork: Another common challenge to effective care planning is the perception that the nursing care plans are merely administrative tasks rather than clinically relevant tools. Furthermore, when care plans are treated as the documentation requirement to satisfy the regulatory practice, they become disconnected from the bedside practice. Thus, this perception is often reinforced when the care plans are poorly integrated into the Electronic Health Records (EHR) systems or when nurses receive limited feedback on how care plans influence the patients’ outcomes.
- Over-Reliance on Templates: Many standardized care plan templates are widely used to enhance efficiency and consistency in the documentation. While the templates can be valuable sharing points, over-reliance on them can pose a significant risk to individualized care. Moreover, the generic templates may fail to capture the unique physical psychological, cultural, and social needs of individual patients. When nurses simply select the pre-populated diagnosis and go for the interventions without critical adaptation, care plans lose their patient-centered focus. Also, the excessive standardization can limit clinical creativity and critical thinking, as the care planning requires nurses to analyze the patient responses.
These are some challenges that nurses face while creating the nursing care plan. The good thing is that by effectively applying the best practices, they can overcome these problems without any hitch.
Best Practices for Effective Nursing Care Plans
To overcome these challenges, the nurses and the healthcare organizations must adopt the best practices that focus on clinical relevance, patient-centered care, and ongoing evaluation.
Here is what they need to do:
- Keep the Patient at the Center: Patient-centered care is the foundation of effective nursing care planning. Furthermore, this involves incorporating patient preferences,s values, and cultural beliefs. They should look at their personal goals. When patients are engaged in care planning they are more likely to participate actively in their care and adhere to the recommended interventions. Also, involving patients and families is essential as it fosters shared decision-making and enhances satisfaction.
- Focus on Priority Problems: Effective care plans focus on the most critical patient needs. Thus, the nurses need to follow the clinical frameworks such as Maslow’s hierarchy of needs. Or they can use the ABCs like airway, breathing, and circulation. Even the safety principles can help to discover the life-threatening and high-risk problems at first. Also, addressing the priority issues ensures that nursing interventions are aligned with immediate patient safety and physiological stability. Secondary concerns can then be addressed as the patient’s condition stabilizes/ This prioritization not only enhances outcomes. It also helps nurses manage time and workload more effectively.
- Use Clear Measurable Language: Clear and measurable goals are essential for evaluating the effectiveness of nursing interventions. Vague statements such as improve comfort or enhance mobility do not offer sufficient direction or measurable outcomes. Also, goals should be specific, measurable, achievable, relevant, and time-bound. For example, A patient will report pain 3/10 within 30 minutes of analgesic administration, which provides a clear benchmark for evaluation. Measurable language enhances accountability, supports continuity of care, and strengthens documentation quality.
- Update Care Plans Regularly: Nursing care plans must be dynamic documents that evolve with the patient’s conditions. Also, changes in clinical status, response to treatment, and patient goals should prompt timely updates to the care plan. Regular reviews and revisions ensure that care plans remain relevant and actionable. Incorporating care plan updates into shift assessments reinforces their role as living tools rather than static records.
The Role of Nurse Leaders and Educators
Well, the nurse leaders and educators play a pivotal role in shaping care planning practices. Also, their support and advocacy are essential for creating environments in which care plans are valued and effectively utilized.
Additionally, key leadership responsibilities include reinforcing professional standards for care planning. It also provides ongoing education on evidence-based practices and audits the documentation for quality rather than mere completion. Also, constructive feedback helps nurses understand how to improve the clinical relevance of their care plans.
Future of Nursing Care Plans
Technologies and data analytics are increasingly becoming the future of nursing care planning. Also emerging technologies include AI-assisted care plan recommendations and predictive analytics. They can be applied to improve clinical decision-making through the recognition of patient risks and the provision of evidence-based interventions.
The most effective aspect is that when care plans are integrated with population health metrics, organizations will be able to track trends and assess outcomes as well as support quality improvement efforts. This will be able to assist in lessening the documentation load and enable uniformity within the care environments. The best care plans are still based on the skill of the nurse to analyze the data and understand the patient situation and offer the caring personal attention that the patients need.
Conclusion
This brings us to the end of the guide! Nursing care plans remain a cornerstone of professional nursing practice. Also, when used effectively, they enhance patient safety, improve clinical outcomes, support interdisciplinary collaboration, and strengthen the professional role of nurses within healthcare systems.
Rather than viewing care plans as documentation burdens, nurses and healthcare organisations must reclaim them as powerful clinical tools grounded in evidence. They are mostly driven by patient needs and reflective professional nursing judgment.
Thus, by addressing the existing challenges, adopting the best practices, and embracing the nursing profession, it continues to advance its mission.
